Malpractice is a problem in every area of medicine. But the hospital emergency room is the medical malpractice problem on steroids. Medical negligence occurs on a regular basis in the emergency room and it often has devastating consequences. On this page we will look at medical malpractice lawsuits involve emergency room care and what the average settlement value of ER malpractice cases are.
Malpractice in the Emergency Room
The emergency room is not a forgiving place. There is little margin for error. Mistakes can’t easily be fixed in the ER. Mistakes happen far too often in Maryland hospitals because the emergency patient is not treated quickly. In most emergency room malpractice cases, diagnostic errors are the primary problem. ER doctors routinely fail to accurately and promptly diagnose serious medical conditions and the patient ends up suffering serious injury or even death. Our law firm brings medical malpractice claims on behalf of victims of negligent emergency room care.
What Can Go Wrong In The Emergency Room?
There are about 100 million emergency department visits annually in this country. We rely so much on the ER to provide quality care when we need it the most. Far too often, this goes very wrong. What happens?
The short answer is everything can go wrong in an emergency room setting, many of which could be eliminated if physicians met the ordinary standard of care. Here are some of the most common types of ER malpractice that we see:
- Misdiagnosis: Emergency room doctors can misread test results or misinterpret symptoms, thereby neglecting essential emergency care. For example, it is common for heart attack victims to be treated as patients with gastrointestinal distress. Other common emergency room misdiagnosis malpractice lawsuits involve:
- Pharmaceutical/Medication errors: The wrong drugs can be given because of poor handwriting, poor communication, and simple error. The wrong medication in an emergency room can cause fatal or severe injury.
- Surgical Errors: Surgical errors happen in all types of surgery. Emergency room physicians are not held to the same standard for surgery as specialists; however, they are held to the standard of knowledge and care of other emergency room surgeons. Surgical malpractice includes cutting the wrong part of the body (for example, nicking an artery), failing to diagnose and treat fractures, and leaving sponges or other medical devices in the patient. During surgery, anesthesia errors are also common.
What’s interesting is that most of these errors are not from the ER doctor themselves. One study suggests that ER mistakes were caused by specialist operating in the emergency room, not the emergency physicians.
How Common Is Emergency Room Medical Malpractice?
Emergency room mistakes are depressingly too common and diagnostic errors are the main problem. A study published in the Annals of Emergency Medicine found that emergency physicians accounted for 52% of all reported cases of misdiagnosis resulting in adverse outcomes. This was twice as high as any other area of medical specialty.
The leading causes of diagnostic failures in the ER were found to be: (1) inadequate medical history, (2) incorrect interpretation of test results, and (3) failure to consult. It was reported that ER physicians failed to order proper tests in 93% of cases as they did not realize the test was required, and 52% of the time the physician lacked the knowledge that the test was indicated. Misinterpretation was found to result from inexperience and mistakes in clinical judgment.
How Much are Emergency Room Malpractice Cases Worth?
Our emergency room malpractice lawyers have earned settlements and verdicts for our clients in emergency room error lawsuits. One question victims commonly have is how much compensation they can expect to receive in a settlement payout or at trial? The only way to know the compensation value of your potential lawsuit is to have an ER malpractice attorney collect all the medical records and retain the appropriate experts. At this point, you will have a better understanding of the range of settlement amounts you might see for your case.
On this page, we provide statistics and sample settlements and verdicts in emergency room malpractice cases in Maryland and around the country.
Statistics on the Value of Emergency Room Malpractice Cases
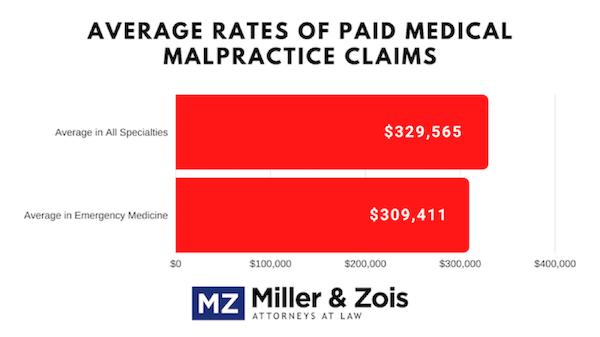
- The average payout for all emergency medicine claims is $330,000. This is right in line with the medical specialties average of $325,000.
- The average settlement or verdict in emergency room malpractice misdiagnosis cases is approximately $362,000. Keep in mind these are payments made by the doctor or, more likely, the malpractice insurer. In 70% of the cases, the doctor gets out of the case on summary judgment, motion to dismiss, or is voluntarily released from the suit. (This statistic is a little misleading. ER doctors are often named in cases because the suit is being filed too close to the statute of limitations so the plaintiffs’ attorneys want to make sure that other defendants are going to blame the emergency room doctors.)
- Misdiagnosis cases are the most common ER mistake claims.
- Acute myocardial infarction emergency room physician malpractice cases that resulted in compensation averaged about $383,000. These are the second most common emergency healthcare provider negligence claims.
- One medical insurer estimates that there are 3.73 claims for every 100,000 emergency department visits and that one-third of these claims will result in a settlement or verdict for the plaintiff. (ER typically pay between < a href=”https://truecostofhealthcare.org/malpractice/” target=”_blank”>$10,000 and $20,000 a year for malpractice insurance.)
- The severity of outcome (death and disability) is the most powerful predictor of both whether a claim will be brought and the settlement value of the case.
Settlements and Verdicts Against Hospital Emergency Departments
Below are recent settlements and verdicts in actual emergency room malpractice cases.
-
- 2023 Illinois – $32,700,000 Verdict: A 25-year-old man visited an emergency room with unexplained foot pain, only to face dire consequences due to alleged medical negligence. Despite presenting with a high-risk profile, the attending physicians failed to promptly diagnose a crucial blood clot. This delay tragically resulted in the amputation of his foot and led to enduring pain, infections, and the necessity for prolonged hyperbaric treatments.
- 2020 New York – $475,000 settlement: A 62-year-old man suffered shortness of breath and chest pain. He presented to the emergency room and came under an ER physician’s care. He was subsequently discharged with no diagnosis. The man later died from a pulmonary embolism. His family alleged negligence against the ER physician. They claimed he failed to timely diagnose a pulmonary embolism. This case settled for $475,000.
- 2020 South Carolina – $1,000,000 verdict: A 66-year-old man fell down several stairs and presented to the emergency room. The man underwent head, neck, and chest CT scans, but the ER radiologist found no abnormalities and discharged the man. Several hours later, the man’s condition worsened. He presented to a different ER. The man was diagnosed with rib and L1 disc fractures. He developed kidney failure and pneumonia and died several weeks later. His family alleged negligence against the radiologist and the ER physician. They claimed the radiologist misinterpreted the CT scans, while the ER physician failed to examine him and order a lumbar CT scan. The defense denied negligence. A jury found the radiologist 90 percent liable and his employer 10 percent liable. They awarded the man’s family $1,000,000.
- 2020 Illinois – $725,000 settlement: A motorcyclist was involved in a collision and went to the emergency room. ER personnel designated the man as a code yellow instead of a code red so he had to wait for admission. The man died from hemorrhagic shock shortly after admission. His family alleged the ER was negligent in failing to timely diagnose his injuries and wrongly designating him as a code yellow instead of a code red. This case settled for $725,000.
- 2019 Maryland – $1,750,000 verdict: A man presented to St. Joseph Medical Center’s emergency room with chest pain and the ER physician failed to perform a CT scan before discharging him. The following day, the man returned to the ER and was diagnosed with an aortic dissection. He underwent an emergency procedure, but died shortly after. The man’s family sued the ER physician for failing to diagnose the aortic dissection initially. The Baltimore City jury awarded $1,750,000.
- 2019 Maryland – $1,300,000 verdict: A 23-year-old man went to the ER with chest pain. His EKG and other test were abnormal but no action was taken. The next morning he suffered a heart attack and later died. His parents alleged negligence against the ER physician. They claimed he failed to timely treat his heart attack, appreciate his symptoms, and consult a cardiologist. The Montgomery County jury awarded $1,300,000.
- 2018 Illinois, $12,000,000 verdict: The plaintiffs sued after their mother died of lung cancer. The gist of their lawsuit was that the defendants, which included the emergency room doctors and specialists, negligently failed to detect lung cancer even though there were several opportunities to do so. As a result, the mother went through extensive chemotherapy and radiation treatment but ultimately passed away from her condition months after the diagnosis. The evidence disclosed that the decedent visited the emergency room with signs and symptoms consistent with pneumonia. The emergency department physician ordered a chest X-ray which was negative for pneumonia and the patient was sent home. The plaintiff contended that approximately one hour later, the radiologist detected an abnormality on the X-ray and asserted that the radiologist should have ordered a CT-scan, which would have diagnosed lung cancer while it was contained within the lung and curable. The plaintiff further asserted that the emergency room physician should have followed up with the radiologist. The emergency room physician maintained that he was never told by the radiologist of the abnormality. The radiologist claimed that he wrote to the emergency room physician and described the abnormality. The plaintiff contended that if diagnosed shortly after the emergency room visit, the cancer clearly would have been a stage 1 tumor which could have been curable through surgery and perhaps some adjuvant treatment. The plaintiff also maintained that although almost a year elapsed before the decedent saw the second primary care physician, the cancer probably could have still been treated successfully, pointing to the absence of symptoms. By the time the decedent received the cancer diagnosis, it had already metastasized to the point where it no longer could be cured. The jury ruled in favor of the plaintiff and awarded $12,000,000.
- 2018 Ohio, $1,900,000 verdict: A woman went to the emergency room for severe pain and died from a pulmonary embolism shortly after being discharged. The family’s lawsuit contended that when the decedent’s mother brought her to the emergency room for leg and buttock pain that had been present for approximately one week which became more severe and the patient developed shortness of breath, the defendant emergency room physician negligently failed to include DVT within the differential diagnosis. The decedent died from a pulmonary embolism five hours after she was discharged. The mother brought the decedent to the emergency room when the decedent complained of particularly severe pain and shortness of breath. She was kept in the ER for about an hour and was discharged with a diagnosis of sciatica. She died from a pulmonary embolism approximately five hours later. The plaintiff asserted that in addition to the history of leg pain and the onset of shortness of breath, risk factors, which included taking birth control medication and obesity, clearly should have prompted the inclusion of DVT within the differential diagnosis. The plaintiff asserted that if this condition was included within the differential diagnosis, it would have prompted testing that would have led to the correct diagnosis and the administration of anticoagulants, preventing the death. The jury believed there was evidence of medical malpractice and awarded the plaintiff $1,900,000.
- 2018 Florida, $456,000 verdict: The plaintiffs brought a wrongful death lawsuit after a woman died from a brain bleed. This wrongful death/medical malpractice action was tried against an emergency room physician and the hospital. The plaintiffs alleged in their lawsuit that the ER doctor negligently failed to order a CT-scan of the brain following the woman’s fall. As a result, her brain bleed was misdiagnosed, leading to his death. The defendants maintained that the decedent suffered a spontaneous brain hemorrhage that did not occur until after she was discharge from the ER. The decedent presented to the emergency room with complaints of left knee pain and facial injuries following a fall. She was seen by the defendant emergency room physician who discharged her with instructions to follow-up with a dentist and her primary care physician. The defendant did not order a CT-scan of the head. Two hours after the discharge, the decedent returned to the emergency room after vomiting and experiencing altered mental status. She was diagnosed with a closed-head injury with resulting subdural hematoma, subarachnoid hemorrhage, infarcts and clots in the brain and a brain herniation. A right craniotomy was performed with tracheostomy placement. The dec
edent was discharged with brain damage for long-term care at another facility where she required 24-hour care. She died 16 months later. The plaintiff’s experts testified that the defendant emergency room physician failed to analyze facial swelling and other signs of head trauma and fell below the required standard in not ordering a CT scan of the decedent’s head. Such a scan which would have diagnosed the decedent’s brain bleed earlier and allowed successful medical intervention, according to the plaintiff’s claims. The defense maintained that a CT scan at the time of the initial presentation would not have detected the condition. The defense also argued that the decedent had a very limited life expectancy. The jury ruled in favor of the plaintiff but awarded only $465,000
- 2017 Oregon, $1,500,000 verdict: A wrongful death action was brought for the death of an adult female college student from meningococcemia on the same day that the emergency room of defendant allegedly evaluated her for complaints of a fever over 103 degrees, chills, shaking, anxiety, low back pain, and body aches. According to the family’s lawsuit, the defendant discharged the decedent from the emergency room after giving her two doses of Tylenol. The decedent’s roommates allegedly found her unconscious in her dormitory around noon later the same day. The estate claimed at the time the physician treated the decedent, the defendant was aware of an ongoing outbreak of meningococcemia that had affected at least three other students at the decedent’s college. The estate claimed the defendant was negligent for failing to consider that the decedent was suffering from meningococcemia, discharging her from the emergency room before ruling out meningococcemia, failing to perform and review a complete blood count before discharging her, failing to draw and review blood cultures, failing to begin antibiotic medications, and failing to have a protocol of clinical care guidelines for evaluating college students presenting with fever and flu-like symptoms during a known outbreak of meningococcemia. The defendant denied liability and claimed that its emergency room physician ordered lab tests and medications, the lab results were unremarkable, and the decedent’s condition improved with treatment. The jury found the defendant’s negligence was a cause of injury and awarded the plaintiff $500,000 for economic damages and $1,000,000 for noneconomic damages.
- 2017, Louisiana $347,000 verdict: The plaintiff reportedly suffered a ruptured appendix that required her to undergo an emergency open appendectomy, and suffered subsequent complications to the surgery, which included pulmonary collapse that required her to undergo oxygenation, post-surgical necrotizing enterocolitis (NEC), systemic inflammatory response syndrome (SIRS) and pneumonia after she was seen by the defendant, an emergency care pediatrician at a hospital emergency room. The plaintiff contended that the defendant had breached the applicable standard of care in treating the patient by failing to diagnose her appendicitis and instead diagnosing her with gastroenteritis. After being diagnosed, she was discharged from the hospital. The plaintiff also contended that the defendant had failed to conduct appropriate diagnostic testing that could have properly diagnosed appendicitis, which included imaging studies, and failed to perform a follow-up comprehensive physical examination of the patient before her discharge, despite the defendant’s discovering several abnormal clinical findings during his initial medical examination of the patient. The defendant denied liability and contended that he had met the applicable standard of care in providing the patient with medical treatment. The defendant contended that at the plaintiff’s initial emergency room visit, imaging studies, such as ultrasounds and/or CT scans, were not warranted because the plaintiff’s condition had improved after he had initially assessed her in the emergency room. The jury reached a verdict for the plaintiffs and awarded the plaintiff with $347,000.
- 2017 Pennsylvania $295,000 verdict: A patient suffered a brain injury resulting in neurological, cognitive, speech and memory deficits after suffering a seizure shortly after two separate visits to an emergency room where she was seen first by the defendants. According to the plaintiff, on her first visit, a few weeks after she was involved in a motor vehicle accident, she presented with symptoms of headache, difficulty concentrating, abnormal lip-smacking, and anxiety but was discharged from the emergency room by the defendant without a diagnosis. Two weeks later, she went to the emergency room with complaints of confusion, headaches, and difficulty sleeping when she was again discharged without a diagnosis. She suffered a catastrophic seizure at home the next day. The plaintiff alleged the defendants were negligent in failing to appreciate her complaints, failing to properly evaluate and examine her, failing to order proper tests or consultations, failing to admit her to the hospital for observation and treatment, and causing a delay in diagnosis. The plaintiff also filed a claim for negligent infliction of emotional distress. The defendants disputed the allegations, arguing the plaintiff had preexisting autoimmune encephalitis that was gradually symptomatic and that she was referred to a neurologist but she did not follow-up with the appropriate specialist. Further, the defendants argued the plaintiff’s claim about emotional distress should be dismissed as he did not witness the alleged negligence of the defendants. The plaintiff was awarded $295,000 for damages and emotional distress.
- 2015: $3.25 Million. Confidential settlement involving malpractice by both doctors and nurses in the emergency room. This is a Miller & Zois case and, regrettably, the details of the case are confidential.
- 2015, Maryland: $3,587,687 Verdict: After being involved in an auto accident, a 64-year-old man is transported to Suburban Hospital. Two ER surgeons provide care to the man, and notice that he previously required neck surgery. His initial examination reveals arm pain and right-hand weakness, leading doctors to diagnose him with a muscle strain. A CT scan is also ordered, which shows a fracture of the right pedicle and vertebrae. The man is discharged, but cannot ambulate on his own. In fact, his family has to call an ambulance to transport him back to the hospital. A subsequent MRI reveals that he actually suffered several disc injuries as a result of the initial accident, requiring emergency surgery. Unfortunately, the damage is already done. The man suffers permanent paralysis of the lower extremities. The man then sues the hospital and the surgeons alleging that the doctors failed to adequately evaluate his condition and that they should have identified the disc injuries on his CT scan. The defendants, on the other hand, suggest that the injury would have happened regardless of their care, or lack thereof. After a 12 day trial, the jury deliberated for 4 hours and found the surgeon and hospital jointly liable for a $3,587,687 verdict.
- 2014, Maryland: $5.2 Million Verdict. Our law firm, Miller & Zois, LLC, handled this case. Our clients suffered a serious knee injury at work. He went5 to the ER and was diagnosed with a sprain and discharged after approximately two hours. He had a knee dislocation. Two days later his leg was amputated. At trial, we argued that the ER doctors missed his injury to the popliteal artery. The case was tried before a Baltimore City jury who did the right thing and gave a fair award.
- March 2013, Maryland: $750,000 Settlement: A 56-year-old man arrives at an emergent care facility with sporadic chest pain. The treating physician orders an EKG that reveals abnormal ST depressions. The man is given a copy of the report and told to go to the emergency room for a cardiac evaluation. While in the emergency room
, the treating physician orders two additional EKGs and reports them as showing a normal sinus rhythm. He schedules the man for a stress test the following week and discharges him. Unfortunately, three days later, the man suffers a fatal heart attack. The plaintiff’s estate sues the hospital for medical malpractice, claiming that the emergency room physician’s negligence was the cause of death, as he failed to obtain a cardiology consultation, even with the abnormal EKG report taken hours before. They claim that had the physician done so, and the patient would have been able to make a full recovery. The parties agree to settle before trial for $750,000.
Contact Miller & Zois About Your Emergency Room Malpractice Case
Our emergency room malpractice attorneys are experienced at identifying the appropriate strategies to maximize the value of these cases. If we accept your case, our primary goal is obtaining maximum compensation for our clients.
If you have been the victim of negligence at a hospital’s emergency department or have lost a loved one from a medical mistake, contact our medical malpractice lawyers at 1.800.553.8082, or online for a free consultation. You will never pay any fees or costs unless we can obtain money damages for you by settlement or at trial.
More Information on Emergency Room Malpractice Claims in Maryland






